Key Takeaways
Uterine fibroids (leiomyomas) are benign growths of the uterine muscle. Many cause no symptoms; others lead to heavy bleeding, pelvic pressure/pain, urinary changes, and fertility challenges.
There are many effective options, from watchful waiting and medications to minimally invasive procedures and hysterectomy. Treatment is personalized and based on your symptoms, goals, and imaging findings.
Certain newer therapies, such as relugolix combination therapy, expand medical options for controlling heavy menstrual bleeding due to fibroids.
If you are in Phoenix, Arizona, Arizona Gynecology Consultants (AZGYN.com) offers advanced imaging and minimally invasive expertise tailored to your goals.
Uterine fibroids (leiomyomas) are noncancerous growths of the uterine muscle. They are very common during the reproductive years, and many cause no symptoms. By midlife, a large share of people will have fibroids, though symptom severity varies. They occur in all racial and ethnic groups; U.S. health-system data show higher diagnosis rates among Black patients and, to a lesser extent, among Hispanic/Latina patients and several Asian subgroups compared with non-Hispanic White patients. These patterns reflect both biology and differences in screening and access to care, so diagnosis rates are not the same as true community prevalence. If you are in Arizona, our team can evaluate symptoms, explain imaging results, and help you choose a treatment that fits your goals.
What Are Uterine Fibroids?
Fibroids are benign (noncancerous) tumors arising from the smooth muscle of the uterine wall. They can occur as a single growth or as multiple growths and may range in size from a seed to grapefruit-sized masses that enlarge the uterus.
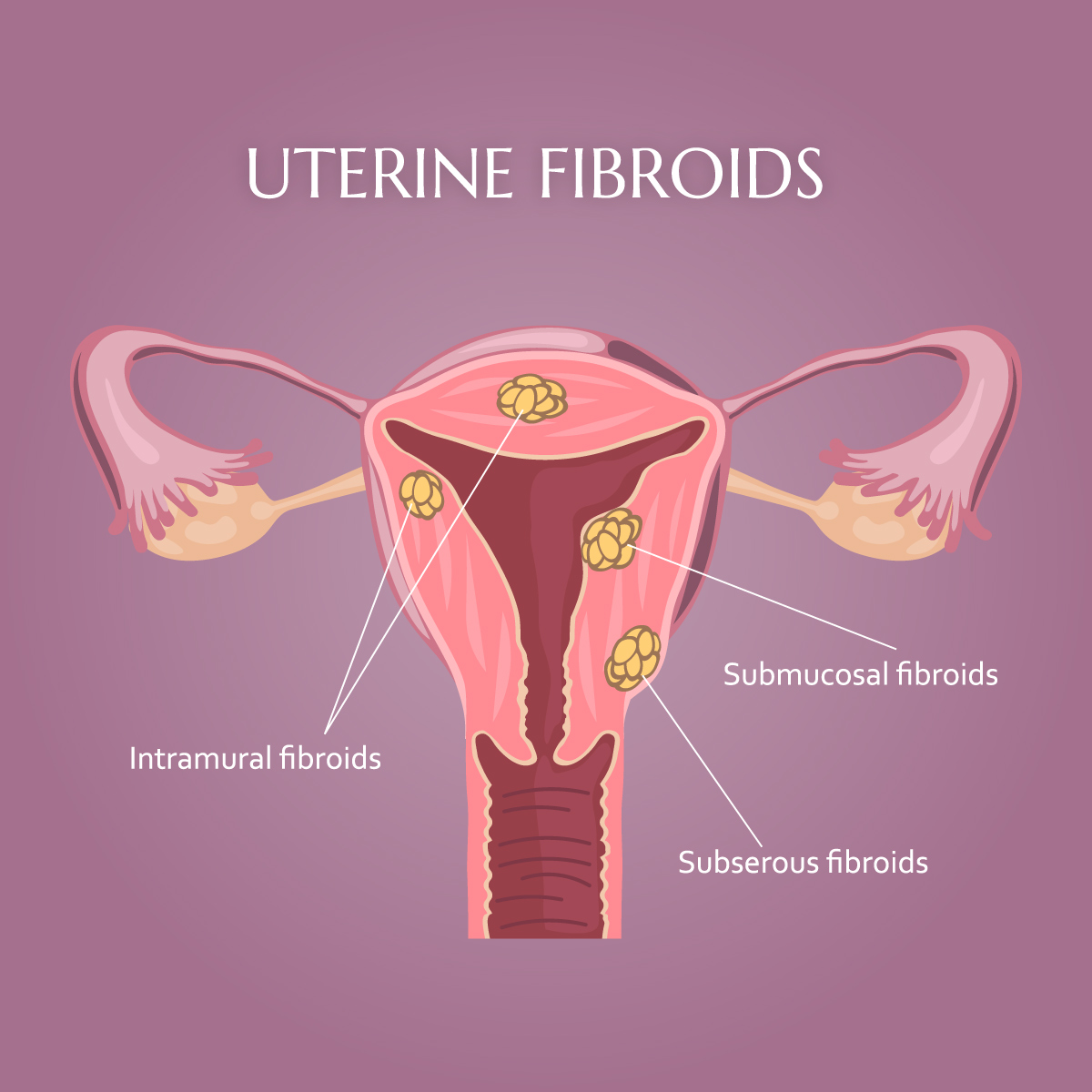
Types of fibroids (by location):
- Intramural: within the uterine muscular wall (most common).
- Submucosal: just beneath the uterine lining; can protrude into the uterine cavity and are often associated with heavy bleeding or fertility issues.
- Subserosal: on the outer surface of the uterus; more likely to cause bulk or pressure symptoms.
- Pedunculated: attached by a stalk, either inside the cavity (submucosal) or outside the uterus (subserosal).
A helpful visual is to think of fibroids as ‘knots’ in muscle tissue, small bulges that can grow within or on the surface of the uterine wall. They push the normal uterine muscle outward as they grow.
How Common Are Fibroids and Who Is at Risk?

Fibroids are among the most common gynecologic conditions. Prevalence increases with age through the 30s and 40s, and significant racial and ethnic disparities exist, with a higher burden among Black women who also tend to develop fibroids at younger ages. Additional risk factors include family history, early menarche, obesity, and possible vitamin D deficiency; research continues to explore biologic and social drivers of these patterns.
What Causes Fibroids?
The exact cause remains unclear, but fibroids are sensitive to estrogen and progesterone. Many fibroids have somatic gene mutations, most commonly in MED12, that are thought to drive growth and influence behavior. Hormonal influences help explain why fibroids often grow during the reproductive years and may shrink after menopause. In the 5-10 years prior to menopause, fibroids can grow more rapidly due to estrogen dominance which is caused by age-related decrease in progesterone. This is often seen with irregular bleeding that worsens during this time of a woman’s life. Another estrogen stimulated disease, such as endometriosis, is found in nearly 50% of women with fibroids.
Signs and Symptoms of Uterine Fibroids
Many people first notice fibroids because of changes in their menstrual cycle or pelvic discomfort. While some fibroids cause no symptoms, others can lead to heavy bleeding, discomfort, or fertility challenges. Recognizing the signs early allows for better management and a wider range of treatment options.
Common Uterine Fibroid Symptoms and Possible Complications
Symptoms depend on size, number, and location. Many people have no symptoms at all.
- Heavy menstrual bleeding (sometimes with clots) or periods longer than 7 days
- Breakthrough bleeding (bleeding outside of the normal cycle time)
- Pelvic pressure or pain; a sense of fullness or abdominal enlargement
- Frequent urination or difficulty emptying the bladder
- Constipation
- Pain with intercourse
- Lower back or leg pain
- Fertility or pregnancy challenges (location-dependent)
Potential complications include anemia from heavy bleeding and, less commonly, acute pain from degeneration (when a fibroid outgrows its blood supply). Seek prompt care for severe pain, lightheadedness, or suddenly heavy bleeding.
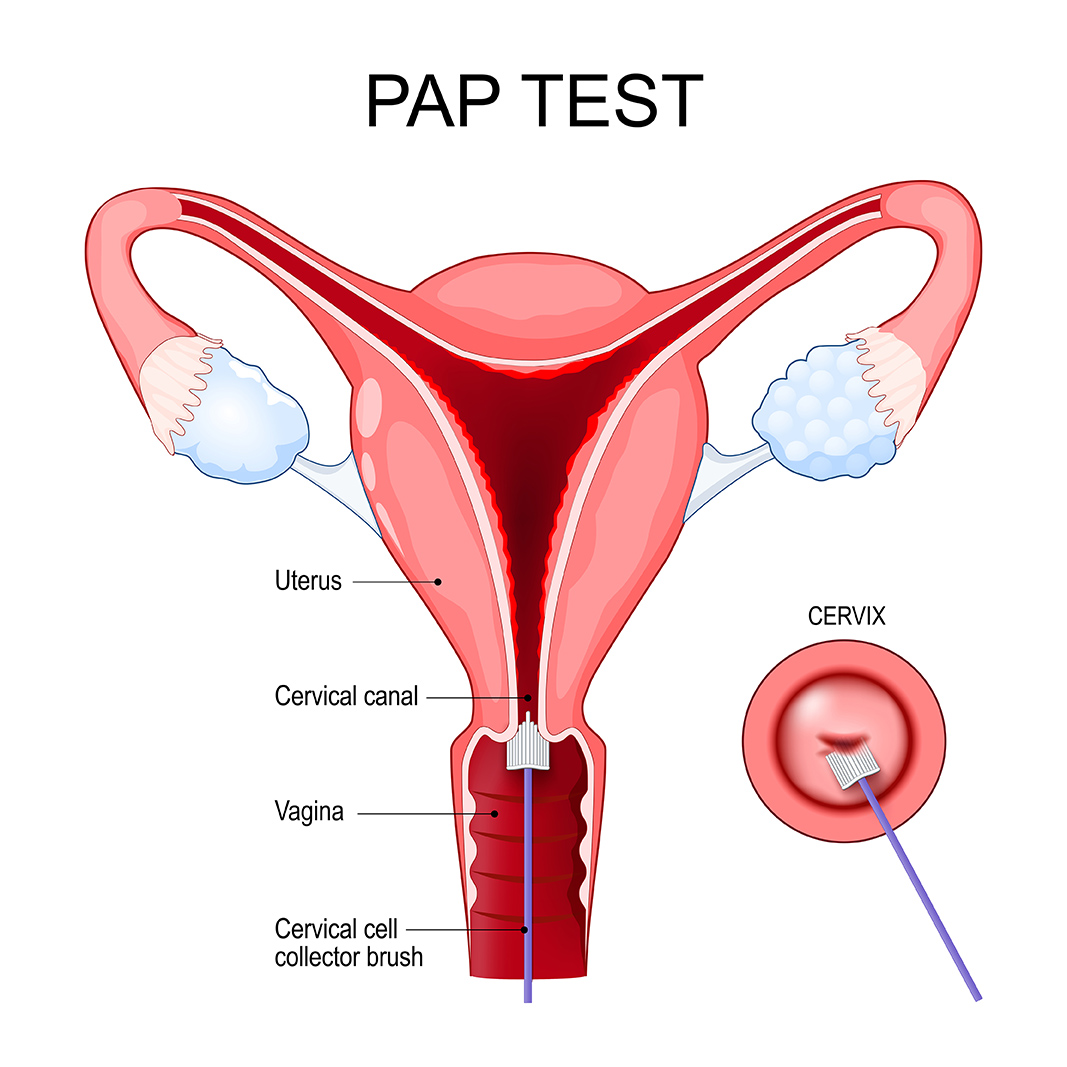
How Are Fibroids Diagnosed?
Diagnosis begins with a medical history and pelvic exam. First-line imaging is typically transvaginal ultrasound because it is accurate, widely available, and does not use radiation. Depending on symptoms and surgical planning, clinicians may use saline infusion sonography to assess the uterine cavity, or magnetic resonance imaging (MRI) to map number, size, and location in complex cases. Laboratory testing such as a complete blood count can evaluate anemia when heavy bleeding is present.
When Should I Seek Treatment?
- Your bleeding or pain affects daily life, work, or emotional well-being.
- You are experiencing increased pelvic pressure, pain with intercourse or protrusion of the abdomen.
- You notice decrease bladder capacity (more frequent urination)
- You are trying to conceive and have been told fibroids might be contributing.
- You are unsure whether your bleeding is normal.
- You have a diagnosis of fibroids and want to understand all options, including minimally invasive and uterine preserving approaches available in Phoenix, Arizona.
Related Reading: What Happens if Uterine Fibroids Go Untreated?
Treatment Options for Uterine Fibroids

There is no single “best” treatment for everyone. The right plan depends on your symptoms, goals (including future pregnancy), fibroid characteristics on imaging, age and overall health. AZGYN emphasizes shared decision-making and minimally invasive options whenever appropriate.
1) Watchful Waiting
If fibroids are small and not causing symptoms, monitoring may be all that is needed, especially near menopause when hormones naturally decline. Your clinician can help track symptoms and repeat imaging if your situation changes. We recommend annual visits, at least, for patients with known fibroids in order to prevent later diagnosis of rapidly growing fibroids.
2) Medications
NSAIDs
Over-the-counter nonsteroidal anti-inflammatory drugs can reduce cramps and menstrual pain, although they do not shrink fibroids.
Tranexamic acid (TXA)
An antifibrinolytic taken only on heavy days, TXA can reduce menstrual blood loss and help lower the risk of anemia. Your clinician will review clotting risk and drug interactions before prescribing.
Hormonal contraception
Combined oral contraceptives and progestin-only methods may regulate cycles and lighten periods. A levonorgestrel intrauterine system – (52 mg) is highly effective for heavy bleeding in appropriate candidates, though it typically does not reduce fibroid size.
GnRH analogs and antagonists
Gonadotropin-releasing hormone (GnRH) agonists and antagonists lower estrogen levels, decreasing bleeding and temporarily shrinking fibroids. Long-term use can be limited by side effects. Therapy duration is generally limited to reduce bone-density risk.
3) Minimally Invasive, Uterus-Sparing Procedures
Hysteroscopic myomectomy
Removes submucosal fibroids through the cervix using a “hysteroscope”, a fiberoptic camera attached to a telescope with a very small channel for intrauterine surgical instruments. It is often ideal when heavy bleeding is the main symptom and a fibroid protrudes into the uterine cavity. It preserves the uterus and can support future fertility when clinically appropriate. It also provides tissue for pathologic analysis.
Laparoscopic or robotic myomectomy
Removes fibroids while preserving the uterus, typically for intramural or subserosal fibroids. Surgery is done through small incisions on the abdomen under general anesthesia. Experienced minimally invasive surgeons discuss incision size, recovery, and recurrence expectations. The usual recovery period is 2-3 weeks. The surgeons at AZGyn are experts in this procedure.
Uterine artery embolization (UAE/UFE)
An image-guided procedure by interventional radiology that blocks blood flow to fibroids, causing them to shrink and improving bleeding and bulk symptoms. Most candidates go home the same day and recover over a few weeks, with symptom relief increasing over weeks to months. Fertility plans, fibroid characteristics, and personal preferences are part of shared decision-making.
Radiofrequency ablation (RFA)
Uterine preserving therapy that uses ultrasound guided heat energy to ablate fibroid tissue. Laparoscopic and transcervical systems are available. Systematic reviews suggest RFA can reduce symptoms and improve quality of life with low complication rates in appropriately selected patients. This is not the same procedure as endometrial ablation (cautery of the lining of the uterus).
MRI-guided focused ultrasound (MRgFUS/HIFU)
A noninvasive technique that focuses ultrasound energy to ablate fibroids under MRI guidance. Relief builds as treated fibroids shrink. Suitability depends on the number, size, and location of fibroids, as well as MRI features. There are limited centers in the US that provide this therapy and the patients that qualify are limited.
4) Hysterectomy (Definitive Treatment)
Because hysterectomy removes the uterus with the fibroids, it permanently resolves bleeding and prevents fibroid regrowth. It can be life-changing for some, especially with very large or recurrent fibroids, but many patients prefer uterus-sparing options. Hysterectomy does not include removal of the ovaries (produce the female hormones) which is commonly misunderstood. Sometimes, removal of the ovaries is done in combination with a hysterectomy if indicated. When a hysterectomy is appropriate, minimally invasive approaches (laparoscopic or vaginal) may shorten recovery for eligible patients. Most patients need 2-3 months for full recovery but often resume many low-stress activities after a couple of weeks. The surgeons at Arizona Gynecology Consultants are experts in all types and approaches for hysterectomy.
How AZGYN Helps You Choose: A Simple Decision Framework
- Your goals: preserve fertility, minimize downtime, avoid hormones, or seek the most durable option.
- Your primary symptoms: bleeding vs bulk/pressure vs pain.
- Imaging details: size, number, and location (submucosal, intramural, subserosal).
- Medical factors: anemia, other conditions, prior surgeries and childbirth.
Tradeoffs: speed of relief, durability/recurrence risk, recovery time, and future pregnancy considerations.

Our clinicians co-create a plan with you, often starting conservatively and progressing to procedural options only if needed, consistent with major guidelines.
Fibroids, Fertility, and Pregnancy
Fibroids can coexist with a healthy pregnancy, but certain types, especially submucosal fibroids that distort the uterine cavity, are more likely to affect implantation, miscarriage risk, or pregnancy course. Before trying to conceive, some patients benefit from myomectomy depending on fibroid size, number, and location. During pregnancy, most fibroids are managed conservatively with symptom control and monitoring; invasive treatment during pregnancy is uncommon and reserved for specific situations. Not all fibroids affect fertility; decisions about surgery before trying to conceive are individualized.
Living With Fibroids: Practical Tips and Emotional Support
- Track cycles and symptoms so decisions are data-informed.
- Address anemia risk with clinician-guided iron therapy if appropriate.
- Exercise, nutrition, and weight management can support overall well-being and help to lower the effects of estrogen dominance; some risk factors such as obesity are modifiable.
- Get regular exams to monitor the size of the fibroids and understand treatment options.
It is common to feel frustrated or overwhelmed. Our team will listen, validate your experience, and help you move forward confidently.
Uterine Fibroids Frequently Asked Questions (FAQ)
If you’ve been diagnosed with uterine fibroids or think you might have them, it’s natural to have questions. Fibroids are common, but every woman’s experience is unique. Whether you’re exploring symptoms, treatment options, or what recovery might look like, we’ve gathered some of the most frequently asked questions to help you feel informed and confident in your next steps.
AZGYN’s Approach to Fibroid Care in Phoenix, Arizona

Accurate diagnosis with advanced in-office ultrasound and access to MRI when needed.
Personalized, minimally invasive fibroid treatment plans with an emphasis on rapid recovery and fertility preservation when possible.
Full spectrum of options: medical therapy; hysteroscopic, laparoscopic, or robotic myomectomy; uterine artery embolization (with interventional radiology partners); radiofrequency ablation; MR-guided focused ultrasound referrals; minimally invasive hysterectomy when appropriate.
At AZGYN, our goal is to help you feel better, faster—with care that fits your body, your goals, and your life. From accurate diagnosis to advanced, minimally invasive treatments, our team is here to guide you every step of the way. If you’re experiencing symptoms or have questions about uterine fibroids, we’re here to help.
Schedule a consultation today and take the next step toward relief and renewed confidence in your health.
Keep Reading to Learn More
Editor’s Note: This article is an updated combination of articles originally published August 5, 2017 and February 15, 2019.
Sources:
American College of Obstetricians and Gynecologists. Management of Symptomatic Uterine Leiomyomas. ACOG Practice Bulletin No. 228. 2021. Accessed October 2, 2025. https://www.acog.org/clinical/clinical-guidance/practice-bulletin/articles/2021/06/management-of-symptomatic-uterine-leiomyomas
Society of Interventional Radiology. The Fibroid Fix: What Women Need to Know. July 8, 2024. Accessed October 2, 2025. https://www.sirweb.org/media/0xhk5umb/sir_2024_fibroid_fix_report_fnl.pdf
U.S. Food & Drug Administration. MYFEMBREE (relugolix, estradiol, and norethindrone acetate) Prescribing Information. Revised 2025. Accessed October 2, 2025. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/214846s012lbl.pdf
U.S. Department of Veterans Affairs, Pharmacy Benefits Management Services. Relugolix, Estradiol, Norethindrone (MYFEMBREE) National Drug Monograph. March 2024. Accessed October 2, 2025. https://www.va.gov/formularyadvisor/DOC_PDF/MON_Relugolix_Estradiol_Norethindrone_MYFEMBREE_Monograph_Mar_2024.pdf
Marsh EE, Wegienka G, Williams DR. Uterine fibroids. JAMA. 2024;331(17):1492-1493. Accessed October 2, 2025. https://jamanetwork.com/journals/jama/fullarticle/2817458
Office on Women’s Health, U.S. Department of Health and Human Services. Uterine fibroids. Updated 2025. Accessed October 2, 2025. https://www.womenshealth.gov/a-z-topics/uterine-fibroids
American College of Radiology. ACR Appropriateness Criteria: Fibroids (Management and Imaging). 2024. Accessed October 2, 2025. https://acsearch.acr.org/docs/69508/Narrative/
Stewart EA, Laughlin-Tommaso SK. Uterine Fibroids. N Engl J Med. 2024;391:1721-1733. doi:10.1056/NEJMcp2309623 Accessed October 2, 2025. https://www.nejm.org/doi/full/10.1056/NEJMcp2309623
Expert Panel on Interventional Radiology (Makary MS, Zane K, Hwang GL, et-al). ACR Appropriateness Criteria® Management of Uterine Fibroids: 2023 Update. J Am Coll Radiol. 2024;21(6S):S203-S218. Accessed October 2, 2025. https://www.jacr.org/article/S1546-1440(24)00263-1/fulltext
National Institute for Health and Care Excellence (NICE). CKS: Menorrhagia (heavy menstrual bleeding) — Tranexamic acid: Prescribing information. Last revised November 2024. Accessed October 2, 2025. https://cks.nice.org.uk/topics/menorrhagia-heavy-menstrual-bleeding/prescribing-information/tranexamic-acid/
Bofill Rodriguez M, Lethaby A, Low C, et-al. Progestogen-releasing intrauterine systems for heavy menstrual bleeding. Cochrane Database Syst Rev. 2020;8:CD002126. Accessed October 2, 2025. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD002126.pub4/full
International Society for Gynecologic Endoscopy. Hysteroscopic myomectomy guidelines. 2023. Accessed October 2, 2025. https://www.isge.org/wp-content/uploads/2023/10/ISGE_Hysteroscopic_myomectomy_The_guidelines.pdf
AAGL Practice Guideline Committee. Evidence-based practice for minimization of blood loss during laparoscopic myomectomy. J Minim Invasive Gynecol. 2025;32(2):113-132. doi:10.1016/j.jmig.2024.09.021. Accessed October 2, 2025. https://www.jmig.org/article/S1553-4650(24)00429-1/fulltext
Society of Interventional Radiology. Uterine fibroids and UFE. Updated September 2024. Accessed October 2, 2025. https://www.sirweb.org/for-patients/conditions-and-treatments/uterine-fibroids/
Chen I, Berman JM, Balk EM, et-al. Radiofrequency ablation for the treatment of uterine fibroids: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2025;32(1):74-91. doi:10.1016/j.jmig.2024.09.011. Accessed October 2, 2025. https://www.jmig.org/article/S1553-4650(24)00416-3/fulltext
Cohen ND, Lin E, Shields JK, Kho KA. Laparoscopic radiofrequency fibroid ablation: a review of current use and future applications. Curr Obstet Gynecol Rep. 2024;13:66-71. doi:10.1007/s13669-024-00382-1. Accessed October 2, 2025. https://link.springer.com/article/10.1007/s13669-024-00382-1
Liu Y, Xiao Z, Luo Y, et-al. Predictive value of contrast-enhanced MRI for the regrowth of residual uterine fibroids after high-intensity focused ultrasound treatment. Insights Imaging. 2024;15(1):274. doi:10.1186/s13244-024-01839-w. Accessed October 2, 2025. https://insightsimaging.springeropen.com/articles/10.1186/s13244-024-01839-w
Practice Committee of the American Society for Reproductive Medicine. Removal of myomas in asymptomatic patients to improve fertility and/or reduce miscarriage rate: a guideline. Fertil Steril. 2017;108(3):416-425. doi:10.1016/j.fertnstert.2017.06.034. Accessed October 2, 2025. https://www.asrm.org/practice-guidance/practice-committee-documents/removal-of-myomas-in-asymptomatic-patients-to-improve-fertility-andor-reduce-miscarriage-rate-a-guideline-2017/
Tzanis AA, Antoniou SA, Gkegkes ID, Iavazzo C. Uterine artery embolization vs myomectomy for the management of women with uterine leiomyomas: a systematic review and meta-analysis. Am J Obstet Gynecol. 2024;231(2):187-195.e1. doi:10.1016/j.ajog.2024.01.014. Accessed October 2, 2025. https://www.ajog.org/article/S0002-9378(24)00044-9/fulltext
Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in Black and White women: ultrasound evidence. Am J Obstet Gynecol. 2003;188(1):100-107. doi:10.1067/mob.2003.99. https://pubmed.ncbi.nlm.nih.gov/12548202/
Roberson ML. The intersection of structural racism and health services research in characterizing the epidemiology of uterine fibroids. JAMA Netw Open. 2024;7(4):e244165. doi:10.1001/jamanetworkopen.2024.4165. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2817008
Mitro SD, Dyer W, Lee C, et-al. Uterine fibroid diagnosis by race and ethnicity in an integrated health care system. JAMA Netw Open. 2025;8(4):e255235. doi:10.1001/jamanetworkopen.2025.5235. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2832108
The post Understanding Uterine Fibroids: Symptoms, Causes, Diagnosis & Treatment Options appeared first on AZGyn.