Generally speaking, we can tell at a glance roughly when a car was produced. Different eras have different trends and their respective signifiers — the 1950s had fins, the 1970s were big and brown, the 1980s were boxy, the 2000s were retro and luxurious (which produced some truly strange designs) — the list goes on. And the cars themselves evolved right along with those times. For instance, despite a Ford Mustang having the same general shape, characteristics, and purpose, a layperson can easily tell that the 2006 and 2026 model years are from different timeframes even if they might not know what timeframes those are, specifically.
But what about cars that have changed so little, or in such minute expressions, that it’s genuinely difficult to tell? There have been many examples of such vehicles over the years, perhaps the most famous of which being the original iteration of the Volkswagen Beetle, still rocking its 1930s-era design up until 2003. A surprising amount of cars followed this trend, in fact: the Fiat 124 / Lada Riva, full-size Jeep SJ Wagoneer, classic Mini, and many others. But most of these went extinct around the turn of the millennium — what about cars that are still in production today?
Obviously, regulations and safety technology has vastly changed between 2006 and today, so let’s exclude things like mandatory backup cameras, interior alterations, and so on — these factors are all compulsory on new cars. Instead, let’s look at the pure design formula: Which cars are fundamentally the same thing, design-wise, from 2006 (model year 2007) to two decades later? There’s quite a few, even some you might see every day.
Chevrolet Express / GMC Savanna cargo van
Jonathan Weiss/Shutterstock
If you want to talk about vehicles that hardly ever change, almost any conversation must start or contain this van. Bluntly speaking, good luck figuring out what year it is without any hints from the VIN plate, because the Chevrolet Express has remained in continuous production through just one generation since 1996. It underwent exactly one facelift, adopting the mid-2000s “cat-eye” GM look in 2003. But aside from minor front fascia changes depending on year and trim, this van has remained fundamentally the same car since its inception. If it isn’t broken, why fix it?
A lot of cargo and fleet vehicles follow this same philosophy, actually. Take for example the Ford Econoline, which ran up to 2013 as a van before Ford replaced it with the Transit in America — you can still buy an E-Series as a cutaway today, and the Transit serves as the basis for most modern budget-friendly camper vans. But the Chevy Express is relatively unique (at least on American roads) for still wearing the same furniture as it did over a decade ago to the point where, apart from what is absolutely mandatory, even the interior is relatively unchanged from the 2000s edition.
That isn’t to say that the 2026 Chevy Express is quite literally the same truck as it was in the 2000s. Despite being built on the same platform with one generation, GM has made incremental improvements throughout its life cycle. Changes such as new engines and transmissions, dashboard designs, safety features, suspension and chassis reinforcements, and more have kept the humble Express thoroughly modernized — though you’d be forgiven for not believing that fact when looking at how they changed on the outside over the years.
UAZ-452 Bread Loaf
Not many automotive designs, period, make it over a half a century without a single substantial exterior change, much less remain in production today. While relatively obscure in the Western world, make no mistake here — this van is the current undisputed champion of anachronisms on four wheels. Known colloquially as the “Bukhanka,” or “Bread Loaf” in Russian, the UAZ-452 began its life in 1958 as the Eastern Bloc’s first serious take on a 4×4 minibus concept.
It was an idea born from the frozen fields of the Eastern Front, with the USSR recognizing the need for a capable, universal military utility truck — basically a halfway point between the Jeep-sized GAZ-69 and larger flatbeds. Bear in mind the landscape that such a vehicle would have to operate in — the Siberian tundra froze over in the winter before thawing into muddy summers. All-terrain capability is effectively a requirement for most Soviet transport and logistics vehicles, and the Bukhanka proved itself particularly well-suited for the job. Its universal body shape could adopt a wide variety of roles, from providing emergency services to serving as a modern overlanding and camping truck.
As for the list of changes over the years, well, the engine is slightly bigger than it used to be — it’s now a 112-horsepower inline-four situated between the driver and passenger. It also received new mirrors and uprated lights, along with certain conveniences like power steering. And that’s basically it; the Bukhanka is, ostensibly, identical in almost every way to its original configuration, and it’s just as capable today as it ever was. It’s easily one of the USSR’s best designs, certainly in comparison to their atomic-powered fever dream of a car.
Toyota Land Cruiser (J70)
At first glance, this entry seems somewhat confusing — the Land Cruiser has evolved far beyond this body style, after all. In fact, the United States’ version of the Land Cruiser is actually the Land Cruiser Prado, with the “true” Land Cruiser is the full-size Lexus LX. And outside the U.S., that beast of an SUV is still called the Land Cruiser. So what’s with the obviously 1980s-era J70? Believe it or not, some markets (including Japan) still field this rugged off-roader nearly unchanged from its 1984 debut, namely those with high demand for a true no-frills off-roader like Australia and South Africa.
The 70-series Land Cruiser was initially launched as the successor to the venerable 40-series, that boxy 4×4 take on the Jeep. It was offered in a wide array of body styles on various wheelbases, a versatility afforded to it by being a body-on-frame design — meaning the body sits on top of a ladder frame, like any other truck. It’s received various updates throughout the years as well, including new engines, transmissions, coil suspension, and more. But the only way to differentiate one year from another at a glance relies upon the front fascia.
Much like the Chevy Express, the J70 Land Cruiser received one major facelift, which updated the front end with newer square headlights, mimicking other 2000s-era Toyotas. However, as of 2024, the J70 has once again reverted to those classic round headlights while keeping a near-identical silhouette to the original. Sure, it’s now got more modern tech inside, but buying this truck in 2026 is genuinely the closest one can get to buying a 1980s 4×4 brand-new — unless you’re in the United States, as it doesn’t meet current U.S. emissions standards.
Jeep Wrangler
This one may draw some ire at first, certainly because the Wrangler underwent a major generational change between the JK’s debut in August 2006 and today. And that’s true; the JK and subsequent JL Wrangler models are quite different under the hood, featuring all-new powertrains, interior designs, upgraded functional items like axles and tires, and so on. They are two different beasts, or more accurately, the JL is an improvement upon the JK’s formula. But then you pass one in traffic, and if it wasn’t for the grille being at a different angle, we’re hard-pressed to find the difference.
Let’s face it: The underlying formula of the Wrangler hasn’t exactly evolved much since the 1940s. At the end of the day, it’s an off-road capable 4×4 with a removable top, foldable windshield, and removable doors; there’s only so many ways you can slice that. But then we look at modern vehicle design trends. Specifically, trucks like the Bronco and (the more modern) Land Cruiser have retro-inspired designs harkening back to the good old days of function before form. The Wrangler never really needed such a refresh; it was, frankly, just always like that.
From the exterior-mounted door hinges to the wide fender flares and the seven-slotted grille to the arrogantly boxy silhouette, it still looks far closer to its late-half 2000s self than most other cars on the road. That certainly doesn’t make the design less characterful, but we must concede that it is basically the equivalent of a different person wearing the same outfit.
Morgan Plus Four
Have you ever yearned for the days when the British roadster was a lightweight, sporty go-kart powered by a peppy four-cylinder with all the safety features of holding a live firework in your hand? Apparently, so too did British carmaker Morgan, so much so that the company simply never stopped production of its rendition: the Plus 4, or Plus Four in modern parlance. And yes, that is an important distinction, because the Plus Four represents a generational leap over the original 1950 Plus 4, which ended production in — ready for it — 2020. Yes, this spritely roadster was in production for 70 years with a single generation.
Fast forward to the modern era, and surely there’s no place for such a car on today’s roads, no? Again, not according to Morgan, which somehow managed to draft a brand-new car that looks nearly identical to the old model and have it pass modern tests enough to sell in the U.S. Granted, this is a coachbuilt car, hand-crafted by a low-volume manufacturer on a per order basis for around the same price as a well-equipped Corvette. This is truly a car for someone who knows exactly what they want and has the means to get it: A brand-new 1950s-era roadster with a warranty sticker.
Much like all of the other vehicles on this list, the Morgan Plus Four satisfies that specific demand — albeit with a smaller customer base — so well that it simply never had to change. Apart from kit cars like a Caterham, this vehicle is truly unique in the enthusiast motoring world, and good luck distinguishing it from the original without looking at the interior or LED headlights.
Uterine fibroids (leiomyomas) are benign growths of the uterine muscle. Many cause no symptoms; others lead to heavy bleeding, pelvic pressure/pain, urinary changes, and fertility challenges.
There are many effective options, from watchful waiting and medications to minimally invasive procedures and hysterectomy. Treatment is personalized and based on your symptoms, goals, and imaging findings.
Certain newer therapies, such as relugolix combination therapy, expand medical options for controlling heavy menstrual bleeding due to fibroids.
If you are in Phoenix, Arizona, Arizona Gynecology Consultants (AZGYN.com) offers advanced imaging and minimally invasive expertise tailored to your goals.
Uterine fibroids (leiomyomas) are noncancerous growths of the uterine muscle. They are very common during the reproductive years, and many cause no symptoms. By midlife, a large share of people will have fibroids, though symptom severity varies. They occur in all racial and ethnic groups; U.S. health-system data show higher diagnosis rates among Black patients and, to a lesser extent, among Hispanic/Latina patients and several Asian subgroups compared with non-Hispanic White patients. These patterns reflect both biology and differences in screening and access to care, so diagnosis rates are not the same as true community prevalence. If you are in Arizona, our team can evaluate symptoms, explain imaging results, and help you choose a treatment that fits your goals.
What Are Uterine Fibroids?
Fibroids are benign (noncancerous) tumors arising from the smooth muscle of the uterine wall. They can occur as a single growth or as multiple growths and may range in size from a seed to grapefruit-sized masses that enlarge the uterus.
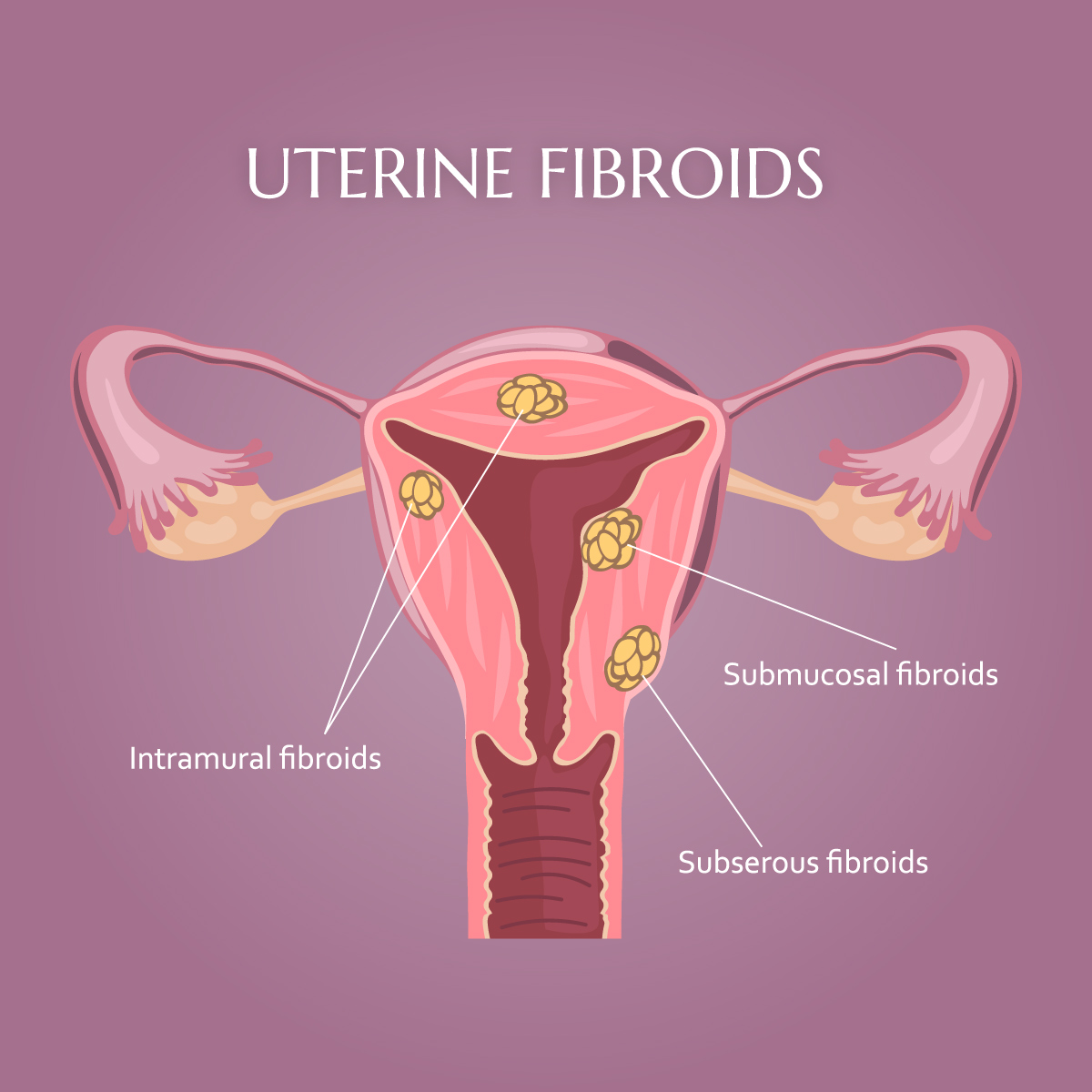
Types of fibroids (by location):
Intramural: within the uterine muscular wall (most common).
Submucosal: just beneath the uterine lining; can protrude into the uterine cavity and are often associated with heavy bleeding or fertility issues.
Subserosal: on the outer surface of the uterus; more likely to cause bulk or pressure symptoms.
Pedunculated: attached by a stalk, either inside the cavity (submucosal) or outside the uterus (subserosal).
A helpful visual is to think of fibroids as ‘knots’ in muscle tissue, small bulges that can grow within or on the surface of the uterine wall. They push the normal uterine muscle outward as they grow.
How Common Are Fibroids and Who Is at Risk?
Fibroids are among the most common gynecologic conditions. Prevalence increases with age through the 30s and 40s, and significant racial and ethnic disparities exist, with a higher burden among Black women who also tend to develop fibroids at younger ages. Additional risk factors include family history, early menarche, obesity, and possible vitamin D deficiency; research continues to explore biologic and social drivers of these patterns.
What Causes Fibroids?
The exact cause remains unclear, but fibroids are sensitive to estrogen and progesterone. Many fibroids have somatic gene mutations, most commonly in MED12, that are thought to drive growth and influence behavior. Hormonal influences help explain why fibroids often grow during the reproductive years and may shrink after menopause. In the 5-10 years prior to menopause, fibroids can grow more rapidly due to estrogen dominance which is caused by age-related decrease in progesterone. This is often seen with irregular bleeding that worsens during this time of a woman’s life. Another estrogen stimulated disease, such as endometriosis, is found in nearly 50% of women with fibroids.
Signs and Symptoms of Uterine Fibroids
Many people first notice fibroids because of changes in their menstrual cycle or pelvic discomfort. While some fibroids cause no symptoms, others can lead to heavy bleeding, discomfort, or fertility challenges. Recognizing the signs early allows for better management and a wider range of treatment options.
Common Uterine Fibroid Symptoms and Possible Complications
Symptoms depend on size, number, and location. Many people have no symptoms at all.
Heavy menstrual bleeding (sometimes with clots) or periods longer than 7 days
Breakthrough bleeding (bleeding outside of the normal cycle time)
Pelvic pressure or pain; a sense of fullness or abdominal enlargement
Frequent urination or difficulty emptying the bladder
Constipation
Pain with intercourse
Lower back or leg pain
Fertility or pregnancy challenges (location-dependent)
Potential complications include anemia from heavy bleeding and, less commonly, acute pain from degeneration (when a fibroid outgrows its blood supply). Seek prompt care for severe pain, lightheadedness, or suddenly heavy bleeding.
How Are Fibroids Diagnosed?
Diagnosis begins with a medical history and pelvic exam. First-line imaging is typically transvaginal ultrasound because it is accurate, widely available, and does not use radiation. Depending on symptoms and surgical planning, clinicians may use saline infusion sonography to assess the uterine cavity, or magnetic resonance imaging (MRI) to map number, size, and location in complex cases. Laboratory testing such as a complete blood count can evaluate anemia when heavy bleeding is present.
When Should I Seek Treatment?
Your bleeding or pain affects daily life, work, or emotional well-being.
You are experiencing increased pelvic pressure, pain with intercourse or protrusion of the abdomen.
You notice decrease bladder capacity (more frequent urination)
You are trying to conceive and have been told fibroids might be contributing.
You are unsure whether your bleeding is normal.
You have a diagnosis of fibroids and want to understand all options, including minimally invasive and uterine preserving approaches available in Phoenix, Arizona.
There is no single “best” treatment for everyone. The right plan depends on your symptoms, goals (including future pregnancy), fibroid characteristics on imaging, age and overall health. AZGYN emphasizes shared decision-making and minimally invasive options whenever appropriate.
1) Watchful Waiting
If fibroids are small and not causing symptoms, monitoring may be all that is needed, especially near menopause when hormones naturally decline. Your clinician can help track symptoms and repeat imaging if your situation changes. We recommend annual visits, at least, for patients with known fibroids in order to prevent later diagnosis of rapidly growing fibroids.
2) Medications
NSAIDs
Over-the-counter nonsteroidal anti-inflammatory drugs can reduce cramps and menstrual pain, although they do not shrink fibroids.
Tranexamic acid (TXA)
An antifibrinolytic taken only on heavy days, TXA can reduce menstrual blood loss and help lower the risk of anemia. Your clinician will review clotting risk and drug interactions before prescribing.
Hormonal contraception
Combined oral contraceptives and progestin-only methods may regulate cycles and lighten periods. A levonorgestrel intrauterine system – (52 mg) is highly effective for heavy bleeding in appropriate candidates, though it typically does not reduce fibroid size.
GnRH analogs and antagonists
Gonadotropin-releasing hormone (GnRH) agonists and antagonists lower estrogen levels, decreasing bleeding and temporarily shrinking fibroids. Long-term use can be limited by side effects. Therapy duration is generally limited to reduce bone-density risk.
3) Minimally Invasive, Uterus-Sparing Procedures
Hysteroscopic myomectomy
Removes submucosal fibroids through the cervix using a “hysteroscope”, a fiberoptic camera attached to a telescope with a very small channel for intrauterine surgical instruments. It is often ideal when heavy bleeding is the main symptom and a fibroid protrudes into the uterine cavity. It preserves the uterus and can support future fertility when clinically appropriate. It also provides tissue for pathologic analysis.
Laparoscopic or robotic myomectomy
Removes fibroids while preserving the uterus, typically for intramural or subserosal fibroids. Surgery is done through small incisions on the abdomen under general anesthesia. Experienced minimally invasive surgeons discuss incision size, recovery, and recurrence expectations. The usual recovery period is 2-3 weeks. The surgeons at AZGyn are experts in this procedure.
Uterine artery embolization (UAE/UFE)
An image-guided procedure by interventional radiology that blocks blood flow to fibroids, causing them to shrink and improving bleeding and bulk symptoms. Most candidates go home the same day and recover over a few weeks, with symptom relief increasing over weeks to months. Fertility plans, fibroid characteristics, and personal preferences are part of shared decision-making.
Radiofrequency ablation (RFA)
Uterine preserving therapy that uses ultrasound guided heat energy to ablate fibroid tissue. Laparoscopic and transcervical systems are available. Systematic reviews suggest RFA can reduce symptoms and improve quality of life with low complication rates in appropriately selected patients. This is not the same procedure as endometrial ablation (cautery of the lining of the uterus).
MRI-guided focused ultrasound (MRgFUS/HIFU)
A noninvasive technique that focuses ultrasound energy to ablate fibroids under MRI guidance. Relief builds as treated fibroids shrink. Suitability depends on the number, size, and location of fibroids, as well as MRI features. There are limited centers in the US that provide this therapy and the patients that qualify are limited.
4) Hysterectomy (Definitive Treatment)
Because hysterectomy removes the uterus with the fibroids, it permanently resolves bleeding and prevents fibroid regrowth. It can be life-changing for some, especially with very large or recurrent fibroids, but many patients prefer uterus-sparing options. Hysterectomy does not include removal of the ovaries (produce the female hormones) which is commonly misunderstood. Sometimes, removal of the ovaries is done in combination with a hysterectomy if indicated. When a hysterectomy is appropriate, minimally invasive approaches (laparoscopic or vaginal) may shorten recovery for eligible patients. Most patients need 2-3 months for full recovery but often resume many low-stress activities after a couple of weeks. The surgeons at Arizona Gynecology Consultants are experts in all types and approaches for hysterectomy.
How AZGYN Helps You Choose: A Simple Decision Framework
Your goals: preserve fertility, minimize downtime, avoid hormones, or seek the most durable option.
Your primary symptoms: bleeding vs bulk/pressure vs pain.
Imaging details: size, number, and location (submucosal, intramural, subserosal).
Medical factors: anemia, other conditions, prior surgeries and childbirth.
Tradeoffs: speed of relief, durability/recurrence risk, recovery time, and future pregnancy considerations.
Our clinicians co-create a plan with you, often starting conservatively and progressing to procedural options only if needed, consistent with major guidelines.
Fibroids, Fertility, and Pregnancy
Fibroids can coexist with a healthy pregnancy, but certain types, especially submucosal fibroids that distort the uterine cavity, are more likely to affect implantation, miscarriage risk, or pregnancy course. Before trying to conceive, some patients benefit from myomectomy depending on fibroid size, number, and location. During pregnancy, most fibroids are managed conservatively with symptom control and monitoring; invasive treatment during pregnancy is uncommon and reserved for specific situations. Not all fibroids affect fertility; decisions about surgery before trying to conceive are individualized.
Living With Fibroids: Practical Tips and Emotional Support
Track cycles and symptoms so decisions are data-informed.
Address anemia risk with clinician-guided iron therapy if appropriate.
Exercise, nutrition, and weight management can support overall well-being and help to lower the effects of estrogen dominance; some risk factors such as obesity are modifiable.
Get regular exams to monitor the size of the fibroids and understand treatment options.
It is common to feel frustrated or overwhelmed. Our team will listen, validate your experience, and help you move forward confidently.
Uterine Fibroids Frequently Asked Questions (FAQ)
If you’ve been diagnosed with uterine fibroids or think you might have them, it’s natural to have questions. Fibroids are common, but every woman’s experience is unique. Whether you’re exploring symptoms, treatment options, or what recovery might look like, we’ve gathered some of the most frequently asked questions to help you feel informed and confident in your next steps.
[/su_spoiler]
Do all fibroids need treatment?
No. If you are asymptomatic and imaging is reassuring, watchful waiting with periodic follow-up is reasonable. Treatment is guided by symptoms, goals, and imaging findings.
What imaging do I need and why?
Ultrasound is first-line for diagnosis and monitoring; MRI or saline infusion sonography may be used to plan procedures or evaluate complex cases.
Can fibroids turn into cancer?
No. Fibroids are benign. A rare cancer called leiomyosarcoma does occur in the uterus, but it is not known to arise from a benign fibroid. Clinicians use your history, exam, and imaging to plan safely.
Will fibroids go away after menopause?
Some fibroids shrink after menopause as estrogen and progesterone levels decline, and symptoms often improve though not always; new or heavy bleeding after menopause should be evaluated.
How fast do fibroids grow?
Growth varies widely: some fibroids remain stable for years, while others enlarge more quickly during the reproductive years or pregnancy; monitoring is individualized. Each fibroid within the same patient’s uterus has its own microscopic make-up and they each function differently from the others.
Do birth control pills make fibroids grow?
Hormonal contraception can help control bleeding but usually does not shrink fibroids and is not known to drive significant growth in most patients.
Which treatments help me avoid surgery?
Depending on candidacy, options include medications (e.g., tranexamic acid, hormonal therapies and GnRH analogs/antagonists). Less invasive therapies such as hysteroscopic myomectomy and transcervical radio frequency ablation of the fibroids are outpatient therapies that allow patients to return to normal activities the following day.
Are there non?hormonal options to reduce heavy menstrual bleeding?
Yes. Tranexamic acid (TXA) taken only on heavy days can significantly reduce blood loss for many patients; your clinician will review safety and interactions.
What’s the difference between myomectomy and hysterectomy?
Myomectomy removes fibroids and preserves the uterus, hysterectomy removes the uterus and is definitive for bleeding due to fibroids.
If I want to get pregnant, which option is best?
It depends on fibroid type, size, and location. Myomectomy is often considered when cavity distorting fibroids are implicated (the fibroids grow into the space that holds the pregnancy). Fibroid ablation can also be considered but the data is limited on the safety for patients that desire a future pregnancy. Endometrial ablation (different from fibroid ablation) is not appropriate if you might desire pregnancy in the future. Many fibroids don’t affect the ability to conceive, and recommendations are tailored to each person’s situation.
Is uterine artery embolization (UFE) a good option if I want children?
UFE can reduce bleeding and pressure, but evidence for future fertility is mixed. When having children is a top priority, myomectomy and sometimes radio-frequency ablation is often recommended because it removes or decreases fibroid size while preserving the uterus. Discuss your goals with your surgeon.
Does MR-guided focused ultrasound (HIFU/MRgFUS) work for all fibroids?
No. Candidacy depends on number, size, location, and MRI features; some patterns respond better than others and careful selection is important. There are limited centers for this procedure.
How long is recovery for common procedures?
Typical recovery is 1-2 days after hysteroscopic myomectomy, about 2–4 weeks after laparoscopic/robotic myomectomy, and a couple of weeks after UFE, RFA, or MRgFUS, though it varies by case.
How fast will I feel better after a procedure?
Timelines vary. Some patients see quicker bleeding reduction after myomectomy or ablation-type therapies, while relief after embolization or focused ultrasound builds over weeks to months as fibroids shrink.
Are vitamins or lifestyle changes enough to treat fibroids?
Healthy weight, exercise, and treating anemia can help overall well-being. Vitamin D is being studied, but supplements do not replace medical or procedural treatments when symptoms are significant.
AZGYN’s Approach to Fibroid Care in Phoenix, Arizona
Accurate diagnosis with advanced in-office ultrasound and access to MRI when needed.
Full spectrum of options: medical therapy; hysteroscopic, laparoscopic, or robotic myomectomy; uterine artery embolization (with interventional radiology partners); radiofrequency ablation; MR-guided focused ultrasound referrals; minimally invasive hysterectomy when appropriate.
At AZGYN, our goal is to help you feel better, faster—with care that fits your body, your goals, and your life. From accurate diagnosis to advanced, minimally invasive treatments, our team is here to guide you every step of the way. If you’re experiencing symptoms or have questions about uterine fibroids, we’re here to help.
Schedule a consultation today and take the next step toward relief and renewed confidence in your health.
AAGL Practice Guideline Committee. Evidence-based practice for minimization of blood loss during laparoscopic myomectomy. J Minim Invasive Gynecol. 2025;32(2):113-132. doi:10.1016/j.jmig.2024.09.021. Accessed October 2, 2025. https://www.jmig.org/article/S1553-4650(24)00429-1/fulltext
Chen I, Berman JM, Balk EM, et-al. Radiofrequency ablation for the treatment of uterine fibroids: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2025;32(1):74-91. doi:10.1016/j.jmig.2024.09.011. Accessed October 2, 2025. https://www.jmig.org/article/S1553-4650(24)00416-3/fulltext
Cohen ND, Lin E, Shields JK, Kho KA. Laparoscopic radiofrequency fibroid ablation: a review of current use and future applications. Curr Obstet Gynecol Rep. 2024;13:66-71. doi:10.1007/s13669-024-00382-1. Accessed October 2, 2025. https://link.springer.com/article/10.1007/s13669-024-00382-1
Liu Y, Xiao Z, Luo Y, et-al. Predictive value of contrast-enhanced MRI for the regrowth of residual uterine fibroids after high-intensity focused ultrasound treatment. Insights Imaging. 2024;15(1):274. doi:10.1186/s13244-024-01839-w. Accessed October 2, 2025. https://insightsimaging.springeropen.com/articles/10.1186/s13244-024-01839-w
Tzanis AA, Antoniou SA, Gkegkes ID, Iavazzo C. Uterine artery embolization vs myomectomy for the management of women with uterine leiomyomas: a systematic review and meta-analysis. Am J Obstet Gynecol. 2024;231(2):187-195.e1. doi:10.1016/j.ajog.2024.01.014. Accessed October 2, 2025. https://www.ajog.org/article/S0002-9378(24)00044-9/fulltext
Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in Black and White women: ultrasound evidence. Am J Obstet Gynecol. 2003;188(1):100-107. doi:10.1067/mob.2003.99. https://pubmed.ncbi.nlm.nih.gov/12548202/
Roberson ML. The intersection of structural racism and health services research in characterizing the epidemiology of uterine fibroids. JAMA Netw Open. 2024;7(4):e244165. doi:10.1001/jamanetworkopen.2024.4165. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2817008
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.